Climbing is hard on your joints, but take care of yourself and you can minimize the damage or at least delay the inevitable.
The post You Climb? You Are Probably Going to Get Arthritis. appeared first on Climbing.
]]>I’m 40 and have osteoarthritis in my fingers. I have the classic symptoms with pain, stiffness, inflammation and bone spurs. I’ve reduced my climbing to one to two days per week and my physical therapist told me to stretch and climb less. Should I give up climbing so my fingers are not completely wrecked when I’m older?
—Bryan Paine
The Doctor Says
Middle age has arrived, and along with it a dark, foreboding presence—the ineluctable path of cellular degeneration. Joint degeneration is the glitch in the matrix of every life styler who uses sport as the medium to experience the world. At some point in your late 30s or early 40s the incumbent idea of continuous progression is ingloriously debunked, and in its place arrives the horrendous notion of slow decline. Hurry up, the roses are dying.
Osteoarthritis is defined by degeneration of the joint surface known as either hyaline or synovial cartilage. Although acute and chronic injury can speed up the onset of osteoarthritis, sport in general is ironically protective even at a fairly intense level. Athletic activity causes cartilage to become more robust and muscles to offer greater stability, thereby affording the joint some resistance. This has been amply demonstrated in runners in particular. If, however, you add a single serious injury—say, an anterior cruciate rupture (the ACL is one of the main stabilizing ligaments in the knee)—you are almost certainly looking down the barrel of earlier degeneration. Translation: Snapping pulleys and ligaments around the fingers will probably not serve you well, nor will chronic damage inflicted by inordinately large mechanical loads on fairly small joint surfaces.
All cells are enfeebled by age-related decay, a state of degeneration due, quite simply, to accumulated cellular assault. Musculoskeletal cells, those in your joints and muscles, are the first to bleep on the radar of perceptible change. Joints become creaky, painful and stiff, and muscles no longer fire as you would like. What starts out as predictable denial will eventually morph into strategic management, whereby you learn to avoid certain aggravating factors in a bid to accommodate those you can’t (or at least don’t want to).
Do-It-Yourself Arthritis Treatments for Rock Climbers
Fish oil. I have many patients with various forms of arthritis, ranging from the more nasty inflammatory types, such as rheumatoid, to the garden variety osteoarthritis, where high doses of fish oils have helped alleviate symptoms, albeit they exude a signature body odor. In reality, current research suggests that a low dose is actually more effective in osteoarthritis (go figure) and has the added benefit of enhanced partner comfort. Get on it!
Glucosamin. The galactic enthusiasm that put glucosamine sulphate (GS) on the shelves of every supermarket virtually overnight has eased somewhat in the last decade, but evidence still firmly points to its ability to ease pain and improve function, with some radiological studies (X-rays) demonstrating that certain GS preparations can slow osteoarthritis progression.
Green Lipped Mussel extract. The eponymous mollusk, derived from a mollusk found on New Zealand shores, may well gezump fish oil in terms of efficacy if the limited research is found to be reliable. Combine them with a dozen oysters, and it will feel like yesteryear!
Snake oil. I recently received a marketing email from a very polite Becky that was titled “Get Your Stiffy Back.” If it seems unbelievable, it probably is! Osteoarthritis is no different to impotence in that desperate people want to believe that the remedy is both easy and fantastic. Conduct your own research with a good dose of skepticism.
Stretching. Simple—a tight joint wears out faster. Stretch joints as if turning your finger into a pretzel. You may find a demonstration video on YouTube somewhere from a time when my voice sounded younger, and I didn’t need to follow my own advice.
Strength. Although strength conditioning sits at the citadel of osteoarthritis management, I doubt too many climbers, in comparison to non-climbers, need to improve their finger strength. A geriatric with knee arthritis, on the other hand, will improve function and slow the progression of osteoarthritis by enhancing leg strength.
Warm up slowly. Creaky joints are usually less so when they are warm. Doubling your warm-up routine will greatly add to your climbing experience, as will pulling on bigger rather than smaller holds. That is, steep juggy routes will typically be less aggravating for tender finger joints than others.
Pain management. Pharmaceutical pain management has its place, but use it as sparingly as possible, and stick with Tylenol-type products rather than anti-inflammatories. The latter have shown to be no more effective and yet come with significantly more potential for serious side effects, namely bleeding in the gastrointestinal tract and heart failure.
Other sports. The simple fact is some people will not be able to climb because finger-joint pain will become prohibitive. In the scheme of bad shit, that’s not so bad. You can try dropping the intensity, but if climbing doesn’t work out, there are other sports that will blow your hair back, if you still have any.
Related:
Dr. Julian Saunders specializes in sports injuries and climbing in particular. He is available for online consultation at http://drjuliansaunders.com/

The post You Climb? You Are Probably Going to Get Arthritis. appeared first on Climbing.
]]>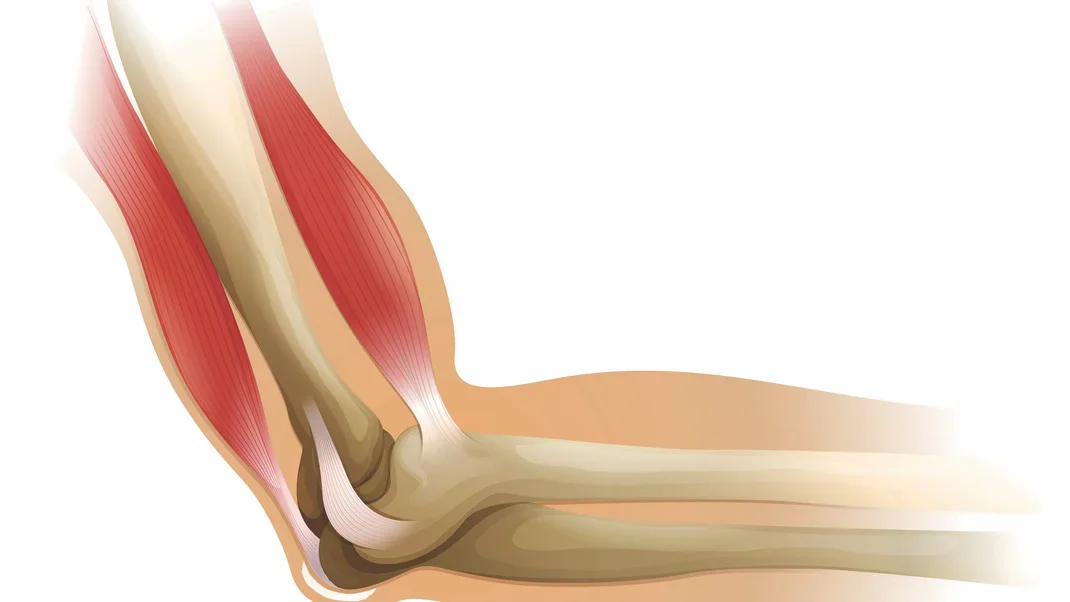
Climber has elbow pain, and of course wonders, "Can I keep climbing?"
The post Injuries and Medical Advice: Not Bursitis appeared first on Climbing.
]]>Q:
My elbow hurts when I lean on it, but outside of that it feels fine. An Internet search points to bursitis, but I don’t have swelling. Are there rehab exercises to alleviate my pain? Could the rehab exercises I’ve been doing for my golf and tennis elbow have caused my recent new problem? My elbow doesn’t hurt when I climb. Can I keep climbing?
—Craig Marcinkiewicz
A:
I’ll wager a hundred buckaroonies that, while you were moving your hand up to the next hold, you banged the tip of your elbow on the hold. You know that moment when everyone watching cringes, and you fall as if you banged into a glass ceiling? Think back. This will have happened sometime in the last six months or so. You will have hit your elbow hard enough to go into a fit of lalochezia and, although the pain subsided at the time, whenever you put the tip of your elbow onto a flat surface the pain grabs you like the searing bite of a Taipan snake.
Just under the skin that covers the back of the elbow (yes, the crusty skin that somehow is much older than the rest of your unblemished hide) lie a bursa and fascia. Under these is bone. This is not olecranon bursitis. I say this because, as you noted, bursitis is inflammatory, and you don’t have swelling.
I don’t know the exact source of pain, or possible combination of bone and soft tissue damage, but I do know that for the next six to eight months resting the tip of your elbow on the table in front of you will elicit pain that requires ninja discipline to tolerate.
There is also the possibility that you fell and decelerated your fall with outstretched arms, causing an avulsion fracture by virtue of your triceps tendon pulling a chunk of bone from the back of your ulnar. Sometimes this injury can be surprisingly painless unless you put pressure on the right spot. A fracture will likely be visible in an X-ray. If you have fractured your elbow, you should talk with a surgeon.
This article appeared in Rock and Ice 243.
The post Injuries and Medical Advice: Not Bursitis appeared first on Climbing.
]]>
Wrist pain following a training injury is probably referred from the climber's palm or forearm. The good news is, you can probably climb.
The post Injuries and Medical Advice: Finger Injuries on a Hangboard appeared first on Climbing.
]]>Q:
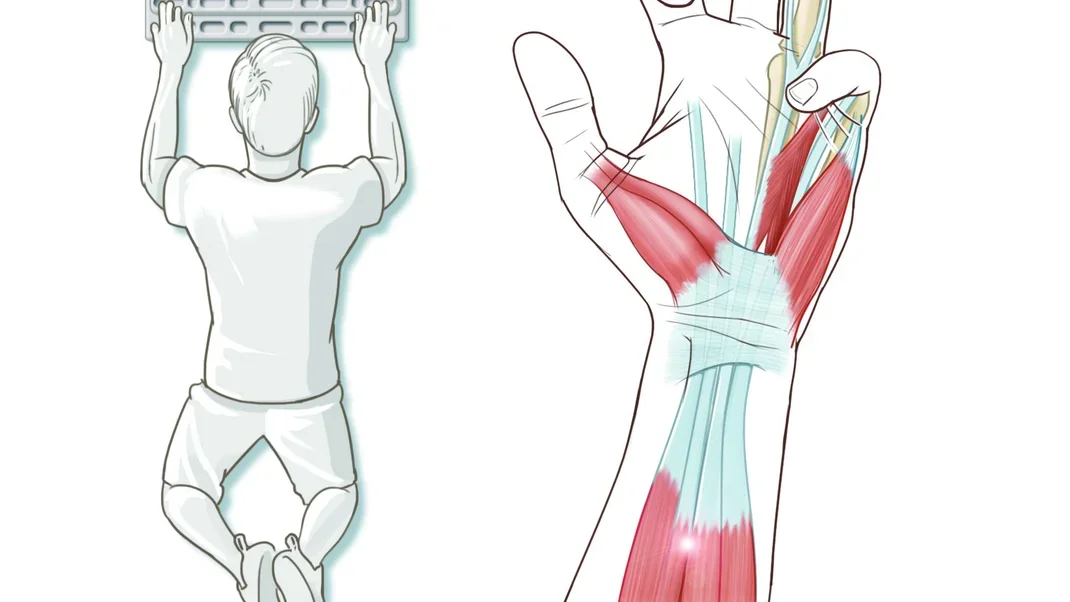
I was hanging on a fingerboard with my index and ring fingers of both hands when I heard a pop and felt a sharp pain. It has been four weeks, and there’s still pain. I have no problem squeezing putty or other climbing/grip-enhancing tools, but occasionally I’ll grab something and feel an intense sharp pain in my wrist, on the opposite side of my thumb. It hurts mildly when I squeeze anything, but is most painful when resistance is applied to my extended ring finger.
—Josh via e-mail
A:
Injuring yourself on the hangboard is deflating. You were not going for glory, you were not in a memorable location with a good mate; there’s no upside, so to speak. But training is usually necessary to get to places you want to go.
Try the Dr. J test, where you pull on each finger in an open-hand position while actively curling the remainder into your palm. My bet is that you will really wince when the little or middle finger is flexed into your palm while you pull on the ring finger, as if pulling on a ring-finger mono pocket. If you are going to have an injury, this is the most likely and preferable one, because you can probably still climb.
One thing is for sure, the pain in your wrist is a neurological ruse and is almost certainly referred from either your palm or your forearm. In your palm the likely source is the fourth lumbrical muscle, but could also be the third palmar interosseous or flexor digiti minimi; without being able to conduct orthopaedic tests, I can’t say which. The pain could also arise from a small tear where the tendons come together at the muscle belly in your lower forearm (two primary muscles, each with four tendons, cause finger flexion).
Again, the good news is that you will likely be able to climb, without pain, as long as you don’t split the neighboring fingers away from your ring finger, such as when you are pulling on a two-finger pocket with your middle and ring fingers and curl the little finger into your palm.
This article appeared in Rock and Ice 235.
The post Injuries and Medical Advice: Finger Injuries on a Hangboard appeared first on Climbing.
]]>
Having strong, well-balanced shoulders is your best chance of a) avoiding the knife, b) climbing anything, and c) a successful surgical outcome.
The post Injuries and Medical Advice: Shoulder Pops appeared first on Climbing.
]]>Q:
I have had shoulder problems since I was 16. Yesterday, my shoulder popped out when my arms were close to the iron-cross position. I am going to go see a sports physician and was wondering if this was the best course of action.
—Michael via online
A:
Michael, sorry, but … your shoulder is phukt. Yes, go and see a sports doc. She will probably get an MRI, refer you to a surgeon, and handball you to a PT. My experience with most manual therapists—PTs, osteopaths and chiropractors—is that they have limited understanding for how to approach recurrent shoulder dislocation. I doubt you will avoid surgery, but your best chance is to find a practitioner who specializes in shoulder rehab.
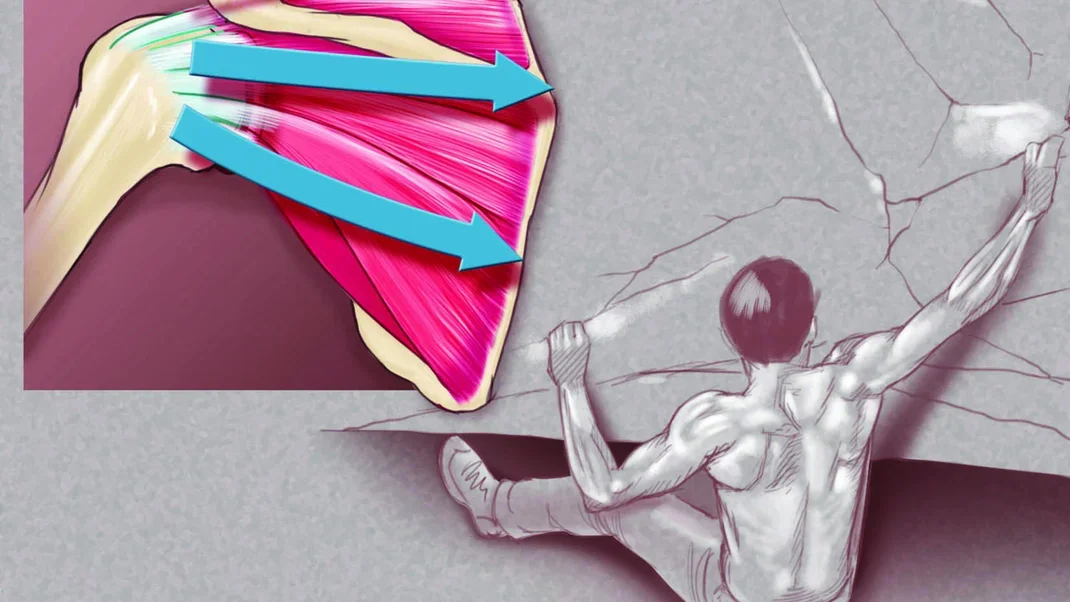
Shoulder stability relies a little on joint architecture (it is a ball-and-socket joint by definition, but imagine a basketball on a tea saucer—it’s rickety), but most of the functional stability arises from ligament restraint and muscle control. There is also a cartilaginous rim around the edge of the socket that affords some further stability without compromising functional range of motion too much.
Instability and dislocation occur when the muscles aren’t strong enough to keep the head of the humerus (basketball) over the glenoid socket (tea saucer). There are genetic factors that predispose you to recurrent dislocation, but for the most part it is born from a single traumatic event that led to your first dislocation.
Having strong, well-balanced shoulders is your best chance of a) avoiding the knife, b) climbing anything that even glances in the general direction of your physical limit, and c) having a successful surgical remedy if you go down that line.
An orthopedist who specializes in shoulder injuries is probably your best chance of finding a therapist who can implement an appropriate exercise program. Controlling recurrent shoulder dislocation is as tricky as Trump’s comb-over. Don’t be shy about trying several options before you commit to one practitioner, since getting a good one will probably save you time, money and mental anguish in the long run.
This article appeared in Rock and Ice 236.
The post Injuries and Medical Advice: Shoulder Pops appeared first on Climbing.
]]>
Leader falls 25 feet and lands directly on her head, setting off a host of injuries.
The post Injuries and Medical Advice: Belayer Hit By Falling Climber, Injures Neck appeared first on Climbing.
]]>Q:
I was belaying when my partner fell 25 feet and landed on my head. My right ear went all the way to my shoulder, and I slammed into the wall, breaking my right arm and two neck vertebrae. I am five weeks into wearing a collar and have pain at various points along my neck when I don’t wear it. I also have bulging discs. I think that rather than sit around, I should be proactive with alignment and muscle strength. Am I correct?
—Rachel Kelley
A:
Holy flying butt-cheeks, Batman! Having someone sit on your head at speed is not how you think you’re going to get a serious injury at the crag.
I broke my neck while surfing a few years back—dived off the front of my board like a complete kook and drilled straight into a sand bank. Every day I get lancing pain that arrives like a renegade ghost rider wielding a samurai-lightning bolt—BOOM! It’s a knee-buckling and entirely unreasonable level of pain. I love it. Why? Because it reminds me that I am not a quadriplegic.
The effects of some injuries will stay with you for life, a little reminder of what can happen, and no less of a reminder of what did not happen. This is one of those times.
Your neck will be a veritable clusterfuck of injuries, fractures being but one. Any neck injury could produce an array of issues that will require significant ongoing management.
In the short term, the collar will give you some relief when your neck becomes tired from holding up your head, but get rid of it as soon as you can—immobilization will only short circuit the longer-term goal of strengthening your neck and regaining movement. How you achieve that is waaaay beyond this column, but suffice to say you seem to be on the right road to recovery. You want a good manual therapist—osteopath, manipulative PT, chiro, whatever pings your pong—as your situation will require close monitoring. Did I mention strength? And range of motion? These are your new best mates. Neglect them and you will know about it.
The pain will subside, given enough time and rehabilitation, and life will resume some ballpark normality, but these injuries, and their downstream effects (such as early joint degeneration), will be with you in perpetuity. Expect aggravations; the sky has not fallen even if the pain seems to be full blast again.
Your injury does unfortunately illustrate an unexpected hazard of belaying and being in a position where the leader can either fall on you or pull you into their flight path. Position yourself out of harm’s way, anchoring to the ground, a tree or other immovable object if necessary.
This article appeared in Rock and Ice 243.
The post Injuries and Medical Advice: Belayer Hit By Falling Climber, Injures Neck appeared first on Climbing.
]]>
A pulley rupture can affect the volar plate and its role in finger flexion. Or is this climbing injury a pulley strain alone? The advice is the same.
The post Injuries and Medical Advice: Volar Plate Strain appeared first on Climbing.
]]>
Q:
I was bouldering, reaching high, thumb down, in an offset crack with the thumb pushing against one side and the fingers pushing against the other. I did the problem and felt fine. Later, my middle finger was stiff and sore around the side when I put pressure on it. Simulating crimping didn’t hurt. A hand surgeon said it was a mild strain of the volar plate. He advised six weeks rest and easing back into climbing (he also recommended finger-buddy taping). Three months later the finger feels better, but tasks that put a bit of pressure to the side can still hurt. MRI needed? Can I ease back into climbing?
— Scott, USA, via e-mail
A:
The volar plate reinforces and stabilizes the palm side of the finger joints and thumb. The structure of the plate and how it interplays with the surrounding pulleys has a little variation that is relevant for climbers, namely that a rupture to the A3 pulley (middle knuckle) can adversely affect how that volar plate articulates in finger flexion.
Damage to the volar plate is typically by way of hyperextension, made more likely with some added axial load; picture a basketball ramming into the end of your finger. This action will result in the plate tearing at its distal insertion point or, alternatively, an avulsion fracture where that insertion pulls off a piece of bone.
The diagnosis of a volar-plate injury is tenuous given the mechanics of an injury, which is far more likely to elicit an A3 pulley strain. In the flexed position that you describe, the pulley is under inordinately more load than the volar plate. Add that you mention pain when pressure is placed more to the side of the finger, where the A3 inserts, and I tend to think the latter injury is more likely.
Ultimately, however, the advice you have been given is good—conservative management rather than surgical. If the pain is only apparent when you put pressure on the area, you should proceed with care. Consider it a warning shot across your bow, and understand that anything potentially aggravating may result in a direct strike. Climbing at a reduced intensity and removing any high-stress training is generally enough to allow the injury to settle down. If the site becomes painful when you pull on the finger, then you have over stepped; back it up, pumpkin! Otherwise, some pain to the type of pressure you describe is categorically normal. I wouldn’t recommend an MRI unless the finger continually aggravates.
This article appeared in Rock and Ice 232.
The post Injuries and Medical Advice: Volar Plate Strain appeared first on Climbing.
]]>
How to maintain while rehabbing: Crimp less (much less), open-hand more, train smart.
The post Injuries and Medical Advice: Tips for Climbing While Rehabbing Your Crappy Elbow appeared first on Climbing.
]]>
1. Crimp less, open-hand more. Crimping loads the wrist flexors more than any other grip position (with the exception of big sloper holds that are common in gyms). The flexor carpi ulnaris is the most commonly afflicted tendon (along with pronator teres). For lateral epicondylosis, avoid pinch-grip training.

2. Train smart. As long as you maintain intensity and duration, fitness can be largely preserved for several months even when you drop training frequency by 80 percent. This huge drop in volume can make healing attainable without you becoming a frump. An exercise physiologist can help you here.
3. Although you may think ongoing use of the campus board will solve the conundrum of what to do with your feet, it may be the one thing you can’t do because it pushes your muscle-strength gains too fast, causing elbow injury. Fingerboards are just as bad.
4. Projecting is great in many regards, but none of them relate to your elbows. As the great Kenny Rogers once sang, “Know when to walk away. Know when to run.” If your elbows are sore, better to run.
5. Cross-training is a great way to create and maintain your strengths without all the usual overloads that cause injury.
6. Buy your Hottie some flowers or a new ice tool, whatever blows his/her hair back—great good can come of such things for reasons less difficult to understand.
This article appeared in Rock and Ice 238.
The post Injuries and Medical Advice: Tips for Climbing While Rehabbing Your Crappy Elbow appeared first on Climbing.
]]>
Given the muscular development and general load put through their forearms, are candidates for nerve-compression syndromes.
The post Injuries and Medical Advice: Carpal Tunnel appeared first on Climbing.
]]>Q:
I feel pins and needles in my first three fingers. I think I have pronator-teres syndrome? Could this be related to using a screwdriver? Climbing?
— Arnie, South Africa
A:
You may have generated pronator-teres syndrome. There is also a chance you will contract leprosy. I have seen pronator-teres syndrome twice in 15 years, but one of my medical comrades has seen leprosy four times in the same period so I am thinking leprosy is twice as common.
I appreciate that climbers, given the muscular development and general load put through their forearms, are candidates for nerve-compression syndromes. The truth, however, is that nerve entrapment in the forearm, and in the arm generally, that could be attributable to climbing is rare.
Numbness in the hand is more likely to be carpal-tunnel syndrome, which is the most common nerve-compression problem in the arm, usually seen in people such as carpenters who use tools all day. Climbing is not a significant catalyst. If you have overt weakness pronating the hand (turning your hand from palm up to palm down while keeping the rest of the arm stationary) then pronator-teres syndrome is somewhat more likely.
Although surgery is an option for carpal-tunnel syndrome, your first port of call should be to a PT; chances are your wrist is rather tight and would benefit from being loosened up. Bracing the wrist usually compounds the problem.
The nerves of the forearm can be impinged at various points. Signs and symptoms that vary from pins and needles as you are feeling to muscle wasting and weakness are grounds for further investigation. A nerve conduction study or an MRI is the investigation of choice.
The post Injuries and Medical Advice: Carpal Tunnel appeared first on Climbing.
]]>
A reader asks whether climbing indoors or in the shade makes climbers susceptible to osteomalacia, or softening of the bones, due to vitamin D deficiency.
The post Injuries and Medical Advice: Sun Deficiency appeared first on Climbing.
]]>Q:
Does climbing indoors or in the shade make us susceptible to osteomalacia due to vitamin D deficiency?
— Pat
A:
Given our vampire-like heliophobia in recent decades, vitamin-D deficiency is a fashionable topic in medical research. To nobody’s surprise, people who shun the sun may not get enough vitamin D. But, much of the chatter has more to do with the economics of your health than your actual health. The supplement industry would rather you buy one of their concoctions than actually do something. Here’s an idea: Instead of popping a pill, catch a few rays of sunlight—along with your daily dose of cutaneous vitamin D synthesis you may even feel a little happier.
True, climbers have been conditioned to avoid the sun, albeit for purposes of friction rather than cancer (the risk of cancer lacks immediacy until the point of diagnosis and as such is a low priority to most). However, by the very nature of going climbing you are likely to catch therapeutic rays as opposed to the office worker who spends much of her day under refrigerator-style-lighting.
Osteomalacia, a condition that results in softening of the bones such that they tend to bend over time, can be caused by vitamin D deficiency. However, unless you spend your winters in Norway and your summers on the dark side of the moon, your vitamin D levels are unlikely to get that low.
Recommended levels of sunlight per day for the purpose of vitamin D synthesis vary from five to 20 minutes depending on, among other factors, how much skin is exposed, sunscreen application (above SPF 8 prevents vitamin D synthesis), time of the day, and the season.
The post Injuries and Medical Advice: Sun Deficiency appeared first on Climbing.
]]>
Nagging wrist pain, origin possibly skateboarding, affects climbing for years.
The post Injuries and Medical Advice: Wrist Pain appeared first on Climbing.
]]>Q:

I have had nagging wrist pain for two years. I bouldered for eight months with occasional aches, and then I started climbing indoors. After a few days of longer, sustained crimping my wrist hurt so badly I ended up sidelined for a year. I returned to climbing, and again my wrist flared up. It can also hurt when I hold a pan or play guitar. I did take a bad fall on an extended wrist while skateboarding three years ago. I’ve had active release technique (ART) therapy, rested and used an arm massager, to no avail.
—Matthew Vanatta, Australia
A:
The skateboarding injury is almost certainly the catalyst of your current situation—falling onto an extended wrist, as most of us are apt to do bouldering, is a recipe for disaster. Trying to guess what is injured sans examination would be laughable. Some educated speculation, however, will at least give you a bit of direction.
One thing is for sure. This is not something that ART or any form of massage is going to fix, though for a small fee I could try some distance reiki. Just send me your credit-card details, and then forget about it.
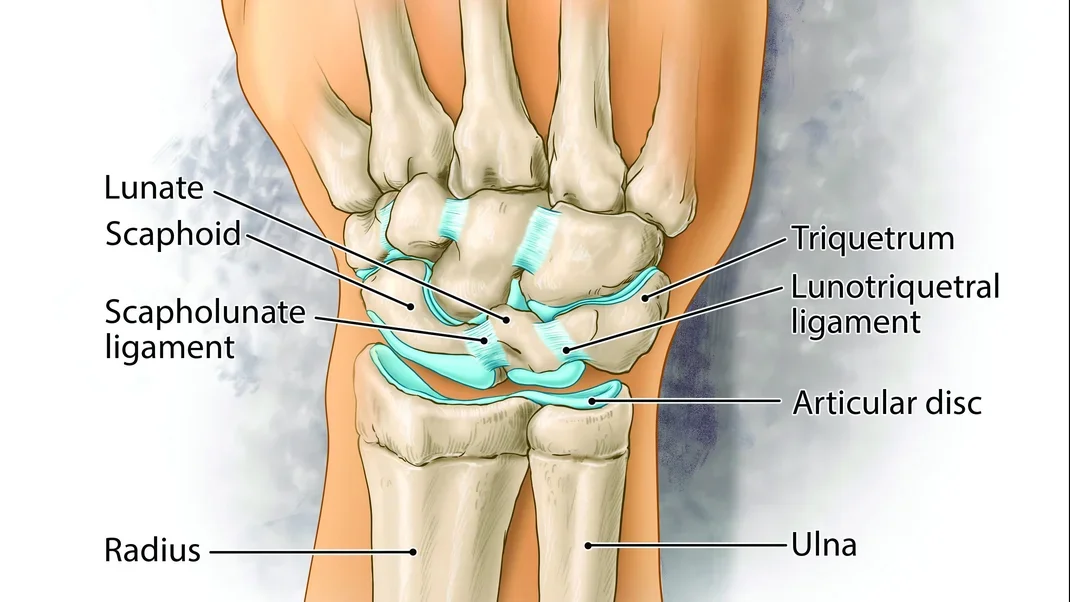
A multitude of things can go wrong, but the big three are fractures (that may not be as obvious as you think), Triangular Fibrocartilage Complex (TFCC) damage, and carpal-ligament rupture. Any one of these can instigate painful and long-lasting downstream problems.
For the most part, the wrist is a mass of bones, cartilage (synovial cartilage on joint surfaces and the TFCC) and ligaments. Tendons, nerves and blood vessels pass through the area, but given your injury mechanism and subsequent presentation, these are probably not contributing.
Most likely you have a combination of TFCC and ligament damage resulting in mechanical mayhem, plus or minus ganglion-cyst formation. Let me again stress that my diagnosis is guess-based. Next stop: MRI!
The post Injuries and Medical Advice: Wrist Pain appeared first on Climbing.
]]>
Q: While desperately manteling a highball 10 years back (I am now 46), I felt my shoulder shift and heard alarming noises. Although I recovered, my shoulder has recently become painful. I had an MRI and saw a surgeon. I damaged the labrum and the bicep, which is cutting through the subscapularis tendon. The surgeon … Continued
The post The Biceps Tendon and Climbing: Why It Blows Out and How to Fix It appeared first on Climbing.
]]>Q:
While desperately manteling a highball 10 years back (I am now 46), I felt my shoulder shift and heard alarming noises. Although I recovered, my shoulder has recently become painful. I had an MRI and saw a surgeon. I damaged the labrum and the bicep, which is cutting through the subscapularis tendon. The surgeon wanted to cut the bicep tendon free at the shoulder and leave it. I have heard it is normal procedure to reattach it. When I saw him a second time and asked about this, he said, “I’m not going into detail until you’ve studied six years of medicine.” I called him a bad name and left. What do you think?
A:
Good on you. Once upon a time doctors, in particular specialists, got away with an expedient “This is very complex and beyond your tiny mind” attitude. Nonsense.
Yours was a very pertinent question and one easily answered. See a more socially adept and communicative practitioner, one that you like and trust. Perhaps Google “stable genius surgeon” and see who you find.
At the top of the arm the bicep tendon runs in a short groove. A small ligament bridging the groove locks the tendon in place. In your case, this ligament has ruptured, and the dislocated tendon is abrading the subscapularis tendon. Imagine a rope running across another rope. The surgeon needs to repair labral damage, stop further delamination of the subscapularis tendon, and release the bicep tendon.
The topic of tenotomy (cutting the tendon) versus a tenodesis (reattachment farther down the shaft of the humorus) is a contentious one among surgeons. Peer-reviewed data indicates that there is little difference in terms of functional outcome—strength, coordination, range of motion—but it is difficult to compare individual studies due to the methodology variables between them, namely surgical techniques. In the instance of a tenotomy, the muscle, once released from the shoulder, bunches above the elbow creating a “Popeye” look. I use several shoulder specialists and they have always opted for a tenodesis.
*****************************************************************************************************************
Q:
I am 50 and have climbed for 30 years. Last year while bouldering I completely ruptured the distal bicep tendon in my left arm. I had the tendon surgically reattached and was climbing six months later and seemed to have made a full recovery after a year. However, I wince every time I grab an undercling. My surgeon said that I wouldn’t have any lingering issues and that I could climb, but I don’t know if he understood the forces that climbing puts on our bodies. So, will I be fine? Is there a scar-tissue time bomb just waiting to go off at the attachment point, or do I have a bionic bicep complete with screws? Should I retire or just lose weight? I hope I don’t have to take up golf. I would never look good in those pants.
–Scott Bouldien, Indianapolis, IN
A:
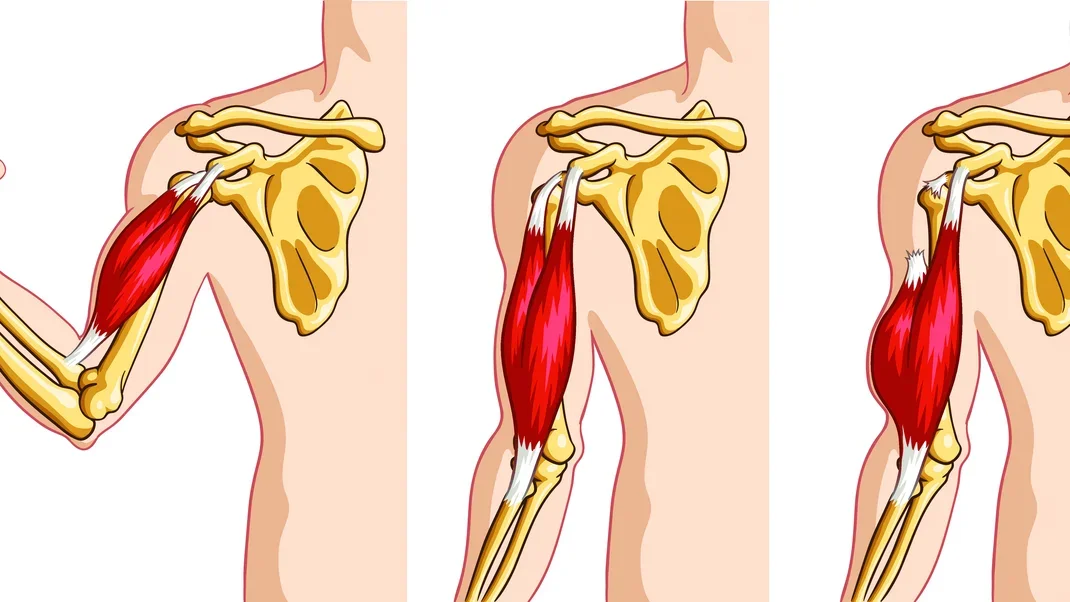
Rupture of the distal bicep tendon, such that it recoils up the inside of your arm toward your shoulder, is not exactly common, afflicting about 1.2 persons per 100,000 each year. It affects mostly men over 30 years of age doing something strenuous, and I dare say that the rate of incidence is somewhat higher if you looked at the climber cohort.
Surgical intervention within a week or so of the injury is the only option if you want full function and strength. A few weeks of “It’ll be fine” will categorically change your options and prognosis. By the time the mounting evidence of pain and dysfunction debunk the entrenched denial, reattachment has become far more complicated, if not prohibitive.
The distal insertion has two attachment points: one to the radius and the other forming a fascial, or soft tissue, attachment just under the skin. All hell breaks loose with a full rupture—popping noises, pain and a bicep that bunches in your arm as it recoils toward your shoulder (called “Popeye Sign” for reasons that do not need explanation).
A year down the track and a whole bunch of rehab (read: climbing) has obviously done you well, i.e., it hasn’t broken again. The issue that is causing you to wince is unlikely to end in another cataclysmic moment. If the tendon has tolerated load for the last six months, any concern about another rupture is probably unfounded.
Turning your hand into a palm-up position while your elbow is flexed, as it is when you undercling, is the primary role of your bicep. Something is getting pinched/tweaked/stretched in your elbow, but it is unlikely to relate to the integrity of the attachment itself. The pain is simply feeding your anxiety that it might! For example, I broke my ankle snowboarding 10 years ago and it can give me some trouble at times, but that doesn’t mean the fracture is in some way still weak or prone to breaking again.
To address some of your other questions: (1) No, you do not have a bionic arm. Only I have bionic arms. They are amazing. You should see them. Hottie says they haven’t changed in 20 years; bless her cotton socks. (2) Retirement is for the half-hearted. (3) If you’re fat, then lose weight—I have never met anyone who regretted it. (4) Golfing attire has a time and a place—I keep a pair of lovely tartan pants just next to my backless chaps.
The post The Biceps Tendon and Climbing: Why It Blows Out and How to Fix It appeared first on Climbing.
]]>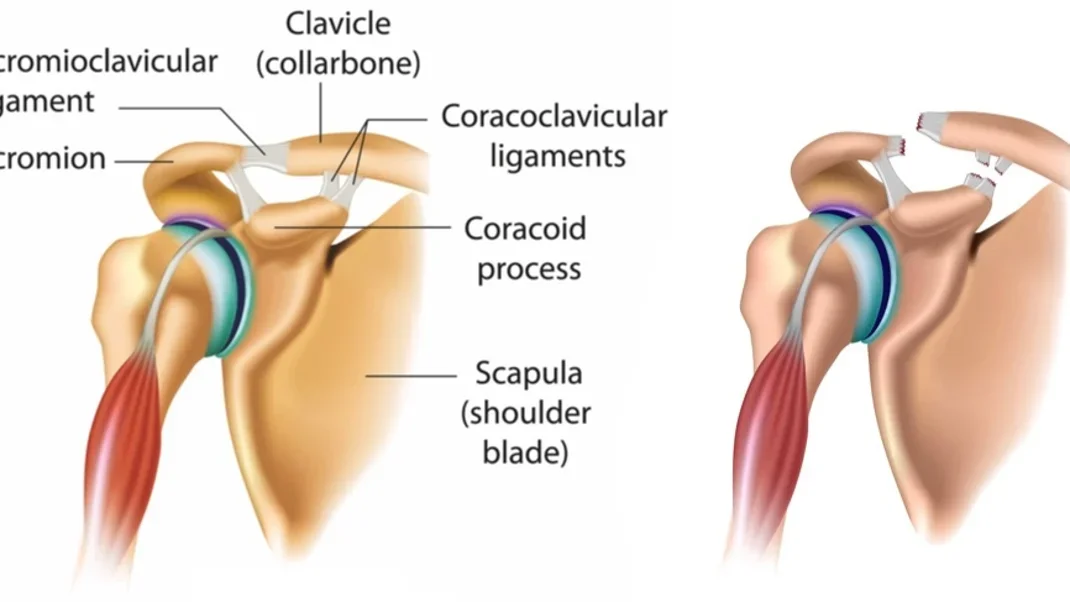
A normal shoulder on the left and, right, one with a ruptured AC joint, an injury commonly known as a separated shoulder. While until recently this injury could end a climbing career, a new surgical procedure involving an implant is often successful. Q: I was skiing and fell onto my shoulder. There is a large … Continued
The post So You’ve Separated Your Shoulder—Now What? appeared first on Climbing.
]]>A normal shoulder on the left and, right, one with a ruptured AC joint, an injury commonly known as a separated shoulder. While until recently this injury could end a climbing career, a new surgical procedure involving an implant is often successful.
Q:
I was skiing and fell onto my shoulder. There is a large lump on top of my shoulder where the collar bone is sticking up. X-rays show that I have damaged my acromioclavicular (AC) joint. Some people suggest surgery while others say it will just heal. What should I do?
—Sam, New Zealand
A:
Here is the issue: Without your AC joint, your arm is only attached to your body by muscle and the singular strut—your collarbone—and stability will be lost. This is a fairly common injury among climbers, not because it’s a climbing injury per se, but because climbers tend be a sportingly diverse bunch whose default mode is full tilt.
There are several ligaments that connect the lateral end of the clavicle to the scapula just beneath it, and these restrain the clavicle and control movement at the AC joint. When you crash onto the tip of your shoulder, say when you fly over the handlebars of a bike, these ligaments are vulnerable. For injuries less than complete rupture, the AC joint remains fairly congruous and injury management is conservative. When all ligaments are severed and the AC joint disrupted, the clavicle tends to pop up creating the appearance of a lump, known as a step deformity, or a “separated shoulder.”
When you raise your arm to the side, the first 90 degrees is handled by the glenohumeral joint. The second 90 degrees, from horizontal to beside your head, occur by way of your scapular gliding across your back. This is where the AC articulation becomes a mission-critical joint since the clavicle acts like a stabilizing rod, enabling the scapular to move with some sense of functional direction.
The first patient I saw with a ruptured AC joint I promptly referred to a surgeon, assuming they will have a technique for relocating this feckless bone. The surgeon sent him back with a note that said something akin to “Woe is Joe, poor sod. His climbing days are done. Nothing I can do. Soz.” Have you ever tried telling that to a climber? Fat-fucking-chance!
In ye olden days, some surgeons would wire the clavicle back in place. Although reattached, there was little flexibility at the AC joint, which arguably caused just as much trouble. In recent years a new operation with a fancy little implant has been quite successful in both reducing the dislocation back into a normal position while retaining some semblance of flexibility as the ligaments heal. This, Nigel, is your future.
The post So You’ve Separated Your Shoulder—Now What? appeared first on Climbing.
]]>